Obstructive sleep apnea is a disorder of sleep related breathing which has increased in prevalence as the epidemic of obesity has increased world-wide. The obstruction occurs in the retropharyngeal space with contributions from nasal obstruction, palatal anatomy, base of tongue prolapse and increased deposition of weight around the neck area. The difference in weight distribution may explain the higher prevalence in middle-aged men (24%) although there is still a relatively high prevalence in women (9%) and less so in children (3%)1 For moderate to severe apnea (which has been linked to the more important medical risks) treatment with nasal Continuous Positive Airway Pressure (CPAP) which maintains the patency of the airway during sleep is very effective although patient compliance can be less than optimal.
EACH APNEA IS ASSOCIATED WITH AN AROUSAL FROM SLEEP TO RESTART BREATHING AND A BRIEF DESATURATION IN THE OXYGEN LEVEL OFTEN REACHING VERY LOW LEVELS. THE AROUSAL OCCURS WITH AN ABRUPT INCREASE IN SYMPATHETIC NERVOUS SYSTEM OUTPUT LEADING TO A GENERALIZED INCREASE IN SYMPATHETIC TONE WHICH MAY CONTINUE DURING THE DAY.
The increased sympathetic tone and hypoxaemia have been linked to a higher prevalence of cardiovascular diseases, particularly hypertension, and metabolic disease including Type 2 diabetes in patients with sleep apnea. As more research is done the relationship between obstructive sleep apnea and other diseases/disorders such as renal function, cancer, mood and cognitive function is being reported.
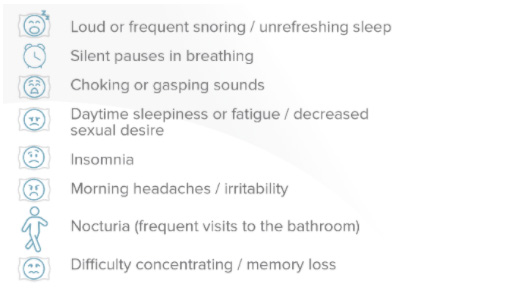
THERE ARE ALSO MORE ACUTE SIGNIFICANT DAYTIME SYMPTOMS CREATED BY THE FREQUENT AROUSALS AND SLEEP FRAGMENTATION. THESE SYMPTOMS ARE TYPICAL OF SLEEP DEPRIVATION EVEN THOUGH, IN THIS CASE, THE HOURS OF SLEEP SEEM TO BE ADEQUATE.
The poorer quality of sleep often results in patients waking up tired and presenting with sleepiness or fatigue throughout the day.
The most common symptom experienced during the day is that of Excessive Daytime Sleepiness (ESD) although it is not an absolute as some patients have 6+no EDS. The importance of the daytime sleepiness in the relationship to other medical disorders is seen in cardiovascular diseases where absence of EDS reduces the cardiovascular risk usually seen in patient with moderate to severe OSA. The reason for the EDS is usually assumed to be related to the degree of severity of the apnea-hypopnea index (AHI) reflecting the number of apneas occurring across the night and thus an indirect measure of the number of times the patient wakes during the night. However, there has been an inconstant relationship reported between the level of EDS and the AHI.
Other more subtle symptoms occurring during the day in patients with OSA include fatigue, poor memory and inability to concentrate – seen as an attention deficit. These dysfunctions can possibly be related to changes in brain structure and function as seen in neuroimaging studies. General changes such as a decrease in cortical metabolism without any overt cognitive deficits have been reported.
STRUCTURAL ATROPHY AND FUNCTIONAL DISTURBANCES OCCUR IN THE RIGHT BA S O L AT E R A L A M Y G DA L A , T H E HIPPOCAMPUS AND RIGHT CENTRAL INSULA. THESE CHANGES CAUSE CHANGES IN EMOTIONAL, SENSORY AND COGNITIVE PROCESSES.
This document will look at the relationship between OSA and those disorders relevant to general adult psychiatric practice – namely depressive symptoms, major depression, cognition and dementia and attention deficit disorder and whether screening for obstructive sleep apnea should become standard practice.
DEPRESSION AND DEPRESSIVE SYMPTOMS
Daytime symptoms expressed by patients with OSA are very similar to those included in the diagnostic criteria for depressive disorder. Patients are tired, have fatigue and feel little pleasure in life, have a low mood, have little energy and battle to concentrate on work or even TV programs. In patients diagnosed with OSA these symptoms are usually explained by the excessive daytime sleepiness which is a common feature. In a psychiatric practice the first diagnosis may be depression rather than OSA.
ANY IMPACT OF OSA ON MOOD MAY IN PART BE DUE TO THE IMPACT OF SLEEP DISRUPTION ON THE FRONTAL CENTRES OF THE BRAIN WHICH ARE ALSO THOSE INVOLVED IN EMOTIONAL MODULATION2. EVIDENCE WOULD INDICATE A CLEAR CONNECTION BETWEEN DISRUPTION OR DEPRIVATION OF SLEEP AND LOSS OF EXECUTIVE FUNCTIONS USUALLY CONTROLLED BY THE FRONTAL OR PREFRONTAL CORTEX.
Typically, patients with depression have insomnia and eat poorly. Some, however, sleep a lot and overeat – symptoms typical of OSA as the hunt for calories in sleepy people has been well-described. Even the presence of insomnia doesn’t exclude the diagnosis of OSA as up to 39% of patients with OSA present with insomnia3.
The relationship between depression and OSA differ depending on the technique or questionnaire used to assess depression or depressive symptoms. When using a standardized psychiatric interview, patients from sleep clinics with OSA show an increased prevalence of depression with women having a higher prevalence than men (29% versus 12%)4. When a score of greater than 10 on the Public Health Questionnaire (PHQ-9) is used 65% of patients with OSA were positive for significant depressive symptoms2. In a reverse strategy of looking for OSA in a patient population already diagnosed with depression the prevalence of OSA has been shown to be up to 14%5. The relationship between OSA and depression may be dependent on the level of daytimes sleepiness as in a community based sample of men the OR for depression was 1.98 overall and increased to an OR of 4.82 in patients with severe OSA when the Epworth Sleepiness Score was over 106.
There is some evidence that patients with OSA are twice as likely to develop depression over a one year follow up than those without OSA – particularly in women where the risk was 2.72 compared to 1.81 in men1. Interestingly, the presence of OSA in patients with depression, particularly if they are male, was shown to lengthen the duration of the initial episode and create resistance to standard anti-depressant therapy (in this case venlafaxine)7.
THE SECOND PART OF THE QUESTION IS WHETHER TREATMENT WITH NASAL CPAP REVERSES THE DEPRESSION OR DEPRESSIVE SYMPTOMS AND HERE THE RESULTS ARE NOT CONSISTENT.
In the study using the PHQ-9 as a diagnostic tool for depression there was a significant reduction in PHQ scores after 3 months of CPAP in men and women2. However, in a meta-analysis using 9 studies which only used the HAM-D scale there was no improvement in that score after using CPAP8. There was, however, a significant improvement in daytime sleepiness and sleep-related quality of life after using CPAP which may contribute to an improved mood.
COGNITION AND DEMENTIA
The cognitive deficit in untreated OSA, such as attention deficits, memory dysfunction, loss of executive functioning and poorer quality of life, are well established relationships and are a real concern to patients. Changes in the functioning of various brain centers, as indicated above, provide clear evidence of the organic nature of such deficits. These deficits are most likely caused by the sleep fragmentation particularly as this feature would disrupt any restorative homeostasis as well as memory consolidative processes which usually occur during sleep. Not surprisingly, the cognitive deficits induced by OSA are much more likely in patients of an older age.
WHEN ASSESSING THE RELATIONSHIP BETWEEN OSA AND COGNITIVE DISORDERS SUCH AS ALZHEIMER’S, A META-ANALYSIS SHOWED A FIVE TIME INCREASE IN OSA AMONGST PATIENTS COMPARED TO HEALTHY CONTROLS9.
The impact of therapy with nasal CPAP is mixed with the effect on cognitive function ranging from not significant8 to partially effective10. In some studies improvements in executive function and memory have been associated with an increase in grey matter in the hippocampus and frontal structure after 3 months of therapy with nasal CPAP11. A residual deficit in cognitive function may indicate a degree of irreversibility in some changes induced by OSA. This is similar to a limited effect of CPAP on metabolic functions compared to a significant effect of CPAP on cardiovascular outcomes.
IT IS, OF COURSE, VERY DIFFICULT TO KNOW HOW LONG ANY PATIENT HAS HAD OSA PRIOR TO DIAGNOSIS BUT ANECDOTALLY MANY PATIENTS REFLECT, AFTER TREATMENT WITH CPAP, THAT THEIR DEFICIT WAS UNRECOGNIZED FOR MUCH LONGER THAN THEY THOUGHT. AS INDICATED PREVIOUSLY THE IMPROVED DAYTIME SLEEPINESS AND QUALITY OF LIFE AFTER CPAP THERAPY MAY INDIRECTLY CAUSE AN IMPROVEMENT IN COGNITIVE FUNCTIONING.
ATTENTION DEFICIT HYPERACTIVITY DISORDER
There is a very clear and well-described relationship between OSA and diagnosed ADHD in children. A systematic review indicated that the prevalence of OSA in children with ADHD (25–30 %) is higher than in the general population (about 3 %)12. Since 2011 clinical practice guidelines for assessment of children with suspected ADHD recommend assessment for OSA13. Subsequent treatment of paediatric OSA by adenotonsillectomy or even nasal CPAP has been shown to significantly reduce ADHD symptoms.
The data on adult patients with ADHD and OSA is limited. In one adult study 19% of patients diagnosed with OSA scored positive for ADHD on the Adult ADHD Self-Report scale14. Patients who were positive for ADHD were also more likely to score higher on the Epworth Sleepiness Scale indicating the strong impact that daytime sleepiness has on cognition.
There are no useful studies investigating the response of the symptoms suggestive of adult ADHD on nasal CPAP therapy apart from a small set of 3 patients in which the ADHD symptoms resolved in 2 of them after CPAP.
OSA SHOULD BE CONSIDERED IN EVERY PATIENT HAVING A PSYCHIATRIC INTERVIEW.
The initial assessment for OSA is easy: ask the patient if they snore. If the answer is positive then the STOP-BANG questionnaire (see box) offers the best screening tool to raise the index of suspicion for obstructive sleep apnea15. A positive answer to 5 or more of the 8 questions indicates an 80% positive predictive value for OSA. A home-based apnea screening test is the most cost-effective way to positively diagnose the severity and impact (oxygen desaturation) of the apnea. A full overnight polysomnogram, often hospital based and therefore expensive, is recommended if multiple pathologies, such as concomitant restless legs syndrome or narcolepsy, are suspected.
If mild OSA is diagnosed then management of the local obstruction – relief of nasal pathology, weight loss or the use of an oral appliance, is required. Moderate to severe obstructive sleep apnea is best managed by use of nasal CPAP which starts with a CPAP titration in order to assess the ability of the patient to manage the CPAP mask and machine as well as check for effectiveness in reducing the number of apneas during sleep.
USUALLY PATIENTS WITH MODERATE TO SEVERE OSA NEED TO USE CPAP LONGTERM UNLESS THEY LOSE A SIGNIFICANT AMOUNT OF WEIGHT WHEN A REPEAT APNEA SCREEN MAY SHOW A REDUCTION OF THE AHI TO NORMAL LEVELS. IF THE AHI CANNOT BE REDUCED TO LESS THAN 20 PER HOUR THEN THE RISK OF FUTURE CARDIOVASCULAR DISEASE REMAINS AND CPAP THERAPY SHOULD CONTINUE.
CONCLUSION
There is evidence for a higher prevalence of OSA than in the general population in adult patients with depression, cognition deficits and attention deficit disorder. The presence of OSA in these disorders leads to incorrect diagnoses and can complicatesthe course and treatment. Thus screening for OSA when assessing patients for these disorders is recommended. The impact of nasal CPAP in reducing symptoms is not consistent and may indicate permanent changes in the brain induced by the hypoxaemia or sleep fragmentation in OSA indicating the urgent need for early diagnosis and treatment. Assessment of the patient after initiation of treatment for OSA is essential to confirm resolution of symptoms.
STOP BANG QUESTIONNAIRE
Click here for the Stop Bang Questionnaire
REFERENCES:
1. Chen Y-H, Keller J, Kang J-H, Hseih H-J, Lin H-C. Obstructive sleep apnea and the subsequent risk of depressive disorder: A population-based followup study. J Clin Sleep Med. 2013; 9: 417-423.
2. Edwards C, Mukherjee S, Simpson L, Palmer L, Almeida O, Hillman D. Depressive symptoms before and after treatment of obstructive sleep apnea in men and women. J Clin Sleep Med 2015; 11: 1029-1038.
3. Smith S, Sullivan K, Hopkins W, Douglas J. Frequency of insomnia reports in patients with obstructive sleep apnoea hypopnea syndrome (OSAHS) Sleep Med. 2004;5(5):449–456
4. Björnsdótter E, Benedikstdótter B, Pack A et al. The prevalence of depression among untreated obstructive sleep apnea patients using a standardised psychiatric interview. J Clin Sleep Med 2016; 12:105-112.
5. Hein M, Lanquart J-P, Loas G, Hubain P, Linkowski P. Prevalence and risk factors of moderate to severe obstructive sleep apnea syndrome in major depression: a observational and retrospective study on 703 patients. BMC Pulm Med 2017; 17:65 doi10.1186/s12890-017-0522-3.
6. Lang C, Appleton S, Vakulin A et al. Associations of undiagnosed obstructive sleep apnea and excessive daytime sleepiness with depression: an Australian population study. J Clin Sleep Med 2017; 13: 575-582.
7. Waterman L, Stahl S, Buysse D et al. Selfreported obstructive sleep apnea is associated with nonresponse to antidepressant pharmacotherapy in late-life depression. Depress Anxiety 2016; 33:1107-1113.
8. Patil SP, Ayappa IA, Caples SM, Kimoff RJ, Patel SR, Harrod CG. Treatment of adult obstructive sleep apnea with positive airway pressure: an American Academy of Sleep Medicine systematic review, meta-analysis, and GRADE assessment. J Clin Sleep Med. 2019;15(2):301–334.
9. Emamian F, Khazaie H, Tahmasian M, et al. The Association Between Obstructive Sleep Apnea and Alzheimer’s Disease: A Meta-Analysis Perspective. Front Aging Neurosci 2016;8:78.
10. Ancoli-Israel S, Palmer BW, Cooke JR, et al. Cognitive effects of treating obstructive sleep apnea in Alzheimer’s disease: a randomized controlled study. J Am Geriatr Soc 2008;56:2076- 81.
11. Canessa N, Castronovo V, Cappa SF, et al. Obstructive sleep apnea: brain structural changes and neurocognitive function before and after treatment. Am J Respir Crit Care Med 2011;183:1419-26.
12. Youssef NA, Ege M, Angly SS, Strauss JL, Marx CE. Is obstructive sleep apnea associated with ADHD? Ann Clin Psychiatry 2011 23:213–224
13. Wolraich M et al for Subcommittee on attention-deficit/hyperactivity disorder, steering committee on quality improvement and management. ADHD: clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics 2011; 128:1007–1022.
14. Hesselbacher S, Aiyer A, Surani S, Suleman A, Varon J. A study to assess the relationship between attention deficit hyperactivity disorder and obstructive sleep apnea in adults. Cureus 2019; 11:e5979 doi:10.7759/cureus.5979.
15. Nagappa M, Liao P, Wong J et al. Validation of the STOP-Bang Questionnaire as a Screening Tool for Obstructive Sleep Apnea among Different Populations: A Systematic Review and MetaAnalysis. PLoS One 2015; DOI:10.1371/journal. pone.0143697
Alison Bentley is a medical doctor, also holding a PhD, and has been involved in the fields of sleep medicine and sleep research for over 30 years. She has held numerous positions on Sleep Societies both local and international. Her practice sees patients with insomnia, obstructive sleep apnea and narcolepsy as well as dealing with childhood sleep disorders. Currently she runs a company which does home-based screening tests for sleep apnea.
Correspondence: dralisonbentley@gmail.com